As a pediatric physiotherapist in Calgary South who specializes in children with gross motor delays and complex neurological or genetic diagnoses, I am often asked how I treat children with these conditions and how it is different from physiotherapy services typically provided in the hospital and school programs. When I tell them I am a Dynamic Movement Intervention (DMI) practitioner the list of questions tends to grow. Let’s discuss these common questions!
What Is DMI Therapy?
Dynamic Movement Intervention (DMI) is used to treat children with motor delays, big or small, by improving their ability to respond to gravity’s demands on their body in various positions and promote progress to developmental milestones. Children actively participate in the exercises of this hands-on therapeutic technique, and exercises are selected based on each child’s specific needs.
As children grow and develop, the neural connections in their brains adapt to the world around them and how they move within that world. This neural connection change is referred to as neuroplasticity and is highest during our younger years. DMI uses this neuroplasticity to help create and strengthen neural connections required to achieve motor milestones.
DMI can also help increase a child’s awareness of their body with the integration of primitive reflexes.
How Do I Know If My Child Will Benefit From DMI?
Many of the families I have worked with over the last few years have frequently commented on the lack of hands-on therapy provided to their children. Parents often feel their child is capable of more than what they are currently doing, or being provided by their current physiotherapist. These families are often eager to learn strategies and tools to better support their child at home or are looking for a skilled and knowledgeable therapist who can provide therapy for their child to take the demand and stress off the parents to provide therapy themselves.
To take the greatest advantage of neuroplasticity, starting therapy young is ideal. However, this does not mean that older children do not benefit from DMI, just that the benefits could occur more slowly. Ideally, once a child begins to present with delays or is diagnosed with a condition that commonly results in delays, DMI therapy should be started. It is easier to proactively work towards preventing poor habits and motor patterns from happening than it is to alter pre-existing and strengthened neural connections that lead to poor movement habits.
I have provided DMI therapy to children all along the gross motor development spectrum. From 6-year-olds who are unable to roll without support, to 3-year-olds who are able to run and jump but experience frequent falls.
What Are the Most Common Conditions Treated With DMI?
Children diagnosed with any type of motor delay may benefit from DMI. Common conditions that I have experience working with include:
Down Syndrome
Cerebral Palsy
Global Developmental Delay
Hypotonia
Spinal cord lesions (Spina Bifida)
Acquired brain injuries
Children do not need a formal diagnosis to receive DMI therapy. Children at risk, such as children who are born prematurely, can also benefit from DMI.
How Long Does DMI Therapy Take to Work?
Some families have seen improvements in head or trunk control in as little as one session, however for strong neural connections to be formed DMI exercises should be performed frequently and on a regular basis. Exercises are taught to families to be performed at home to support a high frequency of DMI provision to a child. As each child and each diagnosis bring their own quirks and complications, it is difficult to provide a firm timeline for the achievement of particular gross motor skills.
Is DMI Painful for My Child?
While it is not uncommon for tears to be shed during the first few DMI sessions, appropriately and skillfully provided DMI therapy is not painful for a child. Many of the children I treat are either non-verbal or have limited communication abilities. Crying is often how these children communicate that an exercise is hard.
Many of the exercises are also challenging for the child as the goal is to build strength, endurance, and skill which requires targeting muscles or movement patterns that are weak. As children become more accustomed to the exercises, the therapist providing the therapy, and the expectation of actively participating they often begin to enjoy themselves and are excited to come for DMI sessions.
Dynamic Movement Intervention is a hands-on therapeutic technique for children with gross motor delays. Children actively participate in exercises specifically selected for their needs and level of function.
DMI stimulates neuroplasticity to create changes in the brain for more optimal movement patterns and to support the development of gross motor milestones. DMI can be provided at any age, however, greater benefits are seen when therapy is started during the first few years of life.
Have you noticed that one shoulder sits higher than the other? Do you find you tend to always lean to one side? Or maybe you’ve noticed that your waist looks fuller on one side, and that your clothes fit a bit funny. You may have something called scoliosis, which is an abnormal curvature of the spine. It can lead to back pain, hip pain, difficulty breathing, poorly fitting clothes, and in some cases, nerve impingement and nerve pain. Read on to learn more.
What Is Scoliosis(1,3)
Scoliosis is a 3D deformation of the spine, which leads to visible changes in the appearance of the torso, and internal structural changes in the intervertebral discs in the back. If left untreated, this eventually leads to irreversible changes in the structure of the bones in the back as well. Depending on the severity of the scoliosis, it may or may not be painful until later adulthood. Typically, most of the structural changes occur during adolescence before the bones are finished growing. Once skeletal maturity is reached – when there can be no more change in bone structure – the curve will remain at that shape. However, later on in adulthood, we can start to experience age-related changes to the bone that can lead to worsening of this curve as time, and age, goes on.
Progression of Scoliosis(1,3)
In adolescence or early stages, scoliosis can be painless, and can often be missed if it is mild. If left untreated and allowed to progress, scoliosis can cause an aching back pain, which typically feels like the muscles on one side of the back are constantly tight. As the scoliosis progresses, you can begin to develop breathing challenges, as the ribcage will be more compressed on one side of the body, making it difficult to take in a full breath. Sometimes, the bottom-most rib can even touch the top of the hip bone on one side which can lead to sharp, acute pain. Over time, the intervertebral discs can become wedged-shaped which can cause nerve complications such as numbness and tingling, nerve pain, and nerve root compression.
What Causes Scoliosis?(1)
80-90% of scoliosis cases are idiopathic – which means there is no known cause. Adolescent Idiopathic Scoliosis is the most common type of scoliosis, affecting adolescents aged 9-17, and typically affects girls more than boys. The remaining 10-20% of scoliosis causes are due to congenital abnormalities (from birth), neuropathic or neuro-muscular conditions, or other systemic diseases.
Because of this sequelae, early detection and treatment is essential to maintaining a quality of life that is not dictated by the scoliosis!
How Can I Check if I Have Scoliosis?(1)
Perform this quick checklist to see if you may have scoliosis:
Is one shoulder or shoulder blade higher than the other?
Is one arm farther away from the body?
Does your body look tilted to one side?
Are your hips uneven in height or twisted?
Is one leg shorter than the other?
Do you find it hard to take a full deep breath?
When exercising, do some moves feel easier on one side of the body?
Do you have consistent achy pain on one side of the upper or lower back only?
Is there a hump on one side of your back when you bend forward?
Do your lower ribs stick out in front on one side of your body?
Does one foot turn in/out more than the other?
If you answer yes to one or more of these questions, you would benefit from a physiotherapy assessment to determine whether you have scoliosis.
A physiotherapist will also be able to help figure out whether your scoliosis is functional or structural.
If you have functional scoliosis, you may answer yes to some of the screening questions above and appear to have a curvature, however on x-ray, the spine remains straight. That is because functional scoliosis is due to muscle imbalances and postural habits, rather than the structure of the spine itself. For this reason, this type of scoliosis responds very well to orthopaedic physiotherapy treatments.
Structural scoliosisinvolves visible changes to the vertebrae on x-ray, and the shape of the spine is physically deformed. Physiotherapy treatments are also very beneficial for structural scoliosis, however depending on the severity, you may also require bracing and/or surgery.
Treatment of Scoliosis
1. Physiotherapy (1,3)
Traditional Orthopaedic Physiotherapy treatment typically consists of core stabilization exercises combined with appropriate back strengthening. The goal is to stretch the tight muscles on the inside of the curve, and strengthen the elongated muscles of the outside of the curve, while also working on the deep core unit to provide overall stability to the whole body. An exercise program will be developed based on your symptoms, and will aim to address areas of pain and stiffness that you are experiencing.
Schroth Therapy is a specific exercise-based approach to treating scoliosis and other postural dysfunctions. The exercises combine postural corrections with breathing mechanics to work towards curve correction. The overall aim of Schroth therapy is to improve motor control of the body and essentially ‘re-learning’ where straight is. When the scoliosis is detected early, and rapid intervention with Schroth is implemented, correction of the abnormal spine curvatures towards a more normal postural alignment is possible.
2. Bracing (1,2,3)
Depending on the severity of your curve on x-ray, an orthopaedic surgeon who specializes in scoliosis may recommend a full body brace. Sometimes, this can result in a slight straightening of the curve, however this is not the primary goal. The brace is typically worn until skeletal maturity has been achieved, and works to prevent further progression of the scoliosis curves. They are typically prescribed to be worn full time (up to 23 hours per day), and work to provide counter-pressure on the outside of the curves while offloading the fatigued muscles on the inside of the curves.
3. Surgery (2)
If or when scoliosis progresses, it can begin to cause compression of the spinal cord. If it does not respond to more conservative treatments (physiotherapy, exercise and bracing), surgery may be required. The surgery would aim to stop curve progression, reduce the deformity, and maintain/regain balance through the trunk. Surgery typically involves spinal fusion where the bones of the spine are fused with hardware to secure the spine in a straightened position. There are also some newer approaches to scoliosis correction surgery that do not involve fusion, but rather are based on pressure/counter-pressure systems, pulleys, and tethers to gradually straighten the spine.
5 FAQ’s about Scoliosis
1. I have scoliosis, will I have to have spinal surgery?
No! The need for surgery is based on the severity of the curve(s), how much it is impacting your daily life, and how you have responded to non-surgical treatment approaches. Having scoliosis does not necessarily mean you have to have surgery.
2. Will my scoliosis just keep getting worse?
Not necessarily. Once skeletal maturity has been reached, the structural component (the bones visible on x-ray) will not worsen until later adulthood, and even then it is not inevitable. It can appear to worsen due to muscle imbalances, depending on habitual postures, exercise habits, workplace ergonomics, etc. This is where a physiotherapy exercise based approach can be VERY helpful!
3. I was told to just “wait and see” what my scoliosis does before treating it. How long should I wait before seeking treatment for my scoliosis?
The ‘wait and see’ approach is an outdated approach to scoliosis management that we now know is not the way to go. The faster you get treatment, the better your chances are of stopping or slowing the curve progression, and avoid worsening symptoms.
4. Does swimming help manage my scoliosis?
Unfortunately, no. Although swimming is a great exercise for overall health and wellness, it can actually accelerate the progression of the curve, as it encourages the flattening of the thoracic spine. Historically, it was recommended as the “best” exercise for patients with scoliosis, as being in the water eliminates the force of gravity. Originally, it was thought that gravity played a role in scoliosis curve progression. However, we now know that this is untrue and have since advanced our treatment protocols for the condition such as the Schroth method outlined above. This is not to say that people with scoliosis should not swim recreationally, however competitive levels or very frequent participation should be avoided.
5. Does scoliosis only affect females?
Although more common in girls, boys can and do get scoliosis as well. Research shows there is a slightly higher prevalence of scoliosis in gymnasts and ballerinas/dancers, which are historically more female-dominant sports. This is more due to the overuse of one side of the body, or putting the body into positions that promote a flatter spine, rather than having more females in the sports.
What Next?
If you suspect you might have scoliosis, or you have already been diagnosed with scoliosis, check in with a physiotherapist for a spine assessment! Even if you currently don’t have any pain, the sooner you start treatment, the better chance you’ll have to stop the curve progression, avoid more serious symptoms, and potentially decrease the severity of the curve. The Peak Health physiotherapist will be able to assess whether you have functional or structural scoliosis, however, requesting full spine x-rays from your doctor would also be beneficial to get a good look at the true shape of the spine. If you would like to pursue Schroth therapy, an x-ray prior to the assessment is mandatory, as the physiotherapist will need to examine the x-ray images before you attend.
References:
Negrini, S., Donzelli, S., Aulisa, A.G. et al. 2016 SOSORT guidelines: orthopaedic and rehabilitation treatment of idiopathic scoliosis during growth. Scoliosis13, 3 (2018). https://doi.org/10.1186/s13013-017-0145-8
American Association of Neurological Surgeons (n.d.). Scoliosis. https://www.aans.org/Patients/Neurosurgical-Conditions-and-Treatments/Scoliosis#:~:text=Scoliosis%20affects%202%2D3%20percent,occurring%20equally%20among%20both%20genders.
When you’re feeling a little sore, nothing feels better than a regular massage therapy. This ancient practice soothes aches and pains, eases stress, and can even help you feel less tight and more relaxed. That’s because massage therapy involves applying pressure to the body in specific ways to ease tension, soothe sore muscles, and reduce pain.
For many people, massage is a luxury at best or an expensive indulgence at worst. But this popular service is also a type of therapy that can provide benefits above and beyond just feeling nice for an hour or two.
Massage therapy has been shown to have numerous physical and mental health benefits. It can relieve stress, ease tension in muscles after exercise, decrease pain from arthritis or injuries, decrease blood pressure and heart rate, relax the mind and body with general stress relief, help with recovery after an athletic event or strain on your body, help with recovering from surgeries such as joint replacements; it can even help improve your immune response by increasing natural killer cell activity!
Types of Massage Treatment
There are a number of different types of massage therapy which are used for pain relief, stress relief and improved circulation. Some use strong pressure, while others apply a gentle touch. Just a few of them are:
1. Sports Massage
2. Swedish Massage
3. Hot Stone Massage
4. Full-Body Massage
5. Prenatal Massage
6. Trigger Point Therapy
7. Myofascial Therapy
8. Relaxation Massage
9. Aromatherapy Massage
Here are five of the most common conditions that a massage therapist has been proven to help with:
1. Tension Headaches
Tension headaches are caused by build-up of muscle tension in the head, neck, and shoulders, as well as the connective tissue that surrounds them. This can happen when you’re stressed, when you’re sitting at a desk for long periods of time, or when you’re dealing with muscle strains or injuries. One of the benefits of massage therapy is that it reduces tension headaches by relaxing contracted muscles in the head and neck, improving blood flow, and reducing stress. In people dealing with chronic headaches, massage therapy can reduce headache frequency and duration by 50%! Even people dealing with occasional tension headaches can benefit from massage therapy. According to one study, receiving massage therapy as soon as symptoms start is most effective for reducing headache frequency and duration.
2. Lower Back Pain
If you suffer from chronic lower back pain, massage therapy can help ease your aches and pains. To treat lower back pain, massage therapy increases blood flow and reduces swelling in the muscles. It may also help relieve muscle tension, which is a common cause of lower back pain.
One study found that people with chronic lower back pain experienced considerable improvements in function and decreased pain after a 10-week massage therapy program. The researchers suggested that massage therapy may be an effective non-drug treatment option for chronic low back pain. Other studies have also found that massage therapy can help people with acute and chronic lower back pain, as well as people with spinal conditions like degenerative disc disease and spinal stenosis.
3. Depression and Anxiety
People with depression and anxiety often experience high levels of stress, which can lead to feelings of anxiety and even pain. Massage therapy has been shown to help ease these symptoms by lowering stress and cortisol levels in the body. One study found that people with generalized anxiety disorder and depression experienced reduced anxiety and cortisol levels after a 12-week massage therapy program. Although studies suggest that massage therapy should be used in addition to medication for people with severe depression or anxiety, it can be a helpful tool for managing mild to moderate symptoms.
4. Chronic Pain Conditions (Such as Arthritis)
Chronic pain conditions like arthritis often cause continual and intense sensations of discomfort and stiffness. Deep tissue massage can help relieve this pain by increasing blood flow and flexibility in the joints, muscles, and connective tissues. One study found that people with osteoarthritis experienced a reduction in pain after six weekly massage therapy sessions. Another study found that massage therapy can help people with fibromyalgia, a condition that causes widespread pain throughout the body. In a randomized controlled trial, people with fibromyalgia who received massage therapy reported less pain and lower anxiety than those who did not receive the treatment.
5. Constipation and Other Digestive Issues
Massage therapy has been found to help improve bowel function in people with constipation or other digestive issues. It’s thought that massage therapy increases blood flow to the digestive system, which helps break down food, increases movement of the intestines, and stimulates the bowels. One review of studies found that massage therapy has a positive effect on constipation, abdominal pain, and symptoms of irritable bowel syndrome. In fact, for people with constipation, massage therapy was found to be as effective as laxatives.
Final Thoughts
There’s no denying that massage therapy is a powerful tool that can do wonders for your body and mind. From easing chronic pain to reducing stress and anxiety, massage therapy is a great way to take care of both your body and your emotions. Speaking with a massage therapist will give you a better idea of all the ways that massage can improve your quality of life. That said, it’s important to remember that every person responds to massage differently. What might work wonders for one person may not do anything for another.
If you’ve never had a massage before, it can be difficult to know what to expect. Luckily, there are many different types of massage out there, so there’s sure to be something for everyone. Whether you’re in need of a relaxing treat or are looking for a therapeutic treatment, you can find the perfect massage for you atPeak Health & Performance. Call us today for more information about Massage Therapy in Calgary South.
Shoulder pain is one of the most common reasons people see a doctor. The shoulder is a complex joint that has so many moving parts and attachments that it’s no wonder it’s prone to pain and injury. Whether you’re an athlete, work in construction, or simply have a desk job, shoulder pain can strike anyone.
Many people think that if they lift something heavy with their arms or have some other motion that puts stress on their shoulders they will get hurt. However, even everyday activities such as reaching up high, sleeping awkwardly and carrying a purse on one side can cause strain in your shoulders and lead to pain.
Working with a skilled chiropractor can help reduce your pain and speed your recovery so you can get back to doing what you love. Here are some common types of shoulder pain, as well as ways you can relieve your symptoms with chiropractic care.
Shoulder Pain From Daily Activities
If you experience shoulder pain that seems to come out of nowhere, there may be a simple explanation – you’re doing too many activities that put pressure on your shoulder muscles and joints without allowing them time to recover. When you have a muscle injury, it doesn’t heal as quickly as a bone break or sprain, so you can feel the effects for weeks or months as it slowly heals.
The shoulder is a particularly complex joint, with many muscles and ligaments that can become overworked and inflamed through activities that may seem small, like sleeping with your arm over your head or constantly reaching above your head at work. To avoid shoulder pain from daily activities, you need to pay attention to your posture as well as the way you move. Even if you rarely lift anything heavy, you can still cause overuse injuries in your shoulders from poor posture.
This type of soft tissue or connective tissue injury responds well to chiropractic treatment.
Shoulder Pain From Overuse
If you’ve experienced an acute injury like a sports injury or a fall, you’re probably aware of the excruciating pain that comes with it. However, sometimes the pain from an injury doesn’t come until days or weeks later, making it difficult to know what is causing it. Injuries to the shoulder joint can cause acute pain as well as chronic pain.
One common way an injury can lead to chronic pain is through overuse – the same way lifting too much weight causes muscle strains, performing movements that put too much stress on your joints can cause overuse injuries like rotator cuff tendonitis and bursitis.
Rotator cuff tendonitis is the most common form of overuse injury of the shoulder, with research suggesting that it affects up to 40% of the general population at some point in their lives. Rotator cuff tendonitis happens when your rotator cuff muscles become inflamed and swollen, causing them to rub against the joint, which can become painful and cause your whole shoulder to feel stiff and sore. Bursitis, an overuse injury that happens when tiny sacs of fluid around your joints become inflamed, is another common cause of shoulder pain from overuse.
This type of injury also responds well to chiropractic techniques just as joint manipulation, shoulder tendon manipulation and other shoulder pain treatment.
Shoulder Instability and Rotator Cuff Injury
If you experience a sudden onset of pain in your shoulder, your doctor may discover that you have some degree of shoulder instability. This means that your shoulder joint is not as stable as it should be, and is particularly common following a shoulder dislocation. If your shoulder is unstable, you may have to undergo surgery to repair the joint and reattach any torn or stretched muscles or ligaments in order to regain full range of motion.
If your shoulder pain is chronic and accompanied by a feeling that your shoulder may “pop out of joint,” you may have rotator cuff tendonitis–the most frequent cause of shoulder instability, so if your pain is not caused by a specific injury but is instead chronic and causing you problems, this may be the source of your pain. Rotator cuff tendonitis results from overuse, particularly of the supraspinatus and subspinous muscles, which help to stabilize the joint. When these muscles are inflamed and swollen, they can rub against the joint, causing pain and inflammation in the entire shoulder.
Chiropractic care addresses shoulder injuries such as these with a wide range of physical therapy.
Chronic Shoulder Pain
If your shoulder pain is severe and does not ease with time, it may be chronic. Chronic pain means that the pain is long-lasting, lasting longer than six to eight weeks. One of the most common reasons for long-term shoulder pain is an underlying condition like arthritis. If you are experiencing long-term shoulder pain, you should see your doctor to determine if there is an underlying condition that may need treatment.
Overuse injuries like rotator cuff tendonitis can also cause chronic pain. While some cases of tendonitis heal in six to eight weeks, others may take longer. If you have been experiencing shoulder pain for longer than six to eight weeks, it is important to see your doctor to rule out underlying causes such as arthritis.
Shoulder Bursitis
If your shoulder pain is accompanied by redness, warmth, and tenderness in the joint above your shoulder, you may have shoulder bursitis. Bursitis occurs when small sacs of fluid that naturally exist in your joints become inflamed and swollen, causing redness and pain. Bursitis is most common in your knees and shoulders, though it can also affect your elbows and hips.
If you have inflamed and swollen joints in your shoulder, your doctor may diagnose you with subacromial bursitis or supraspinatus bursitis. Bursitis occurs when you have a sudden increase in shoulder movement or you perform repetitive motions that put pressure on your joints or cause friction in the joint. It is common for people who work in construction, sports coaches, and people who work on computers to experience bursitis as a result of their jobs.
Tendon Tears
The rotator cuff is made up of four muscles and a tendon that attaches these muscles to the bones in your shoulder joint. If you suddenly increase the intensity of your workouts, or if you have a degenerative condition that makes it difficult to move your arm normally, you may tear one of these tendons. Tendon tears happen when the tendon becomes overstretched and snaps or separates from the muscles around it. While some tears are minor, others can be quite severe and require surgery to repair.
Conclusion
As you can see, there are many reasons for shoulder pain, from poor posture and repetitive motions to sudden injuries. If you are experiencing shoulder pain, it is important to see your doctor to rule out any underlying causes so you can start to heal. With treatments like chiropractic adjustments and physiotherapy, you can address the root cause of your pain and reduce your discomfort. So don’t suffer in silence if you have shoulder pain – callPeak Health & Performance and get started on care that can relieve your suffering.
When you’re a patient in physiotherapy, the sessions are generally set up to be once-a-week appointments for a certain amount of time. During those appointments, your physiotherapist will dig into whatever issues you’re dealing with that day, whether it’s pain in your knee or weakness in your hip. And then you go home again and have another appointment the following week.
Once you leave your initial period of physiotherapy though, things get trickier. How often should you have physiotherapy from this point onward? Is there an ideal frequency?
To answer this question (and many others like it) we reached out to some experts on the topic: physiotherapists! Here’s what they had to say about how often you should have therapy after finishing your initial sessions:
How often should you have physiotherapy?
This will actually depend on two things: the injury or ailment you’re working on and your physiotherapist’s recommendations. Why the injury? Well, different injuries require different amounts of therapy. A bad sprain, for example, will more likely require longer appointments than a torn rotator cuff.
Why the physiotherapist’s recommendation? Let’s say you have a torn rotator cuff. Your therapist will likely prescribe intensive, longer-term care. However, if you’re back to normal activities after a few weeks, then a few times a month might be sufficient. Once you’ve had an initial assessment, your physical therapist will recommend a treatment plan that matches your physical activity and health condition.
After an injury or episode of pain.
If you’ve just had a spell of pain or an injury that caused you to see a physiotherapist, the best course of action is to continue to have physiotherapy services. This is the perfect time to get some long-term care. You want to keep the therapy going to make sure any lingering issues are treated and that you’re strengthening and stabilizing your injured areas. Most likely, your physiotherapist will want you to come in as often as you can so that you can make the most of the sessions. (If you’re in some sort of work-related pain, though, you’ll want to check with your employer to see if you can take the time to go to therapy. It’s up to your company to decide how much time off is fair.)
To prevent re-injury and strengthen your body.
If you’re just trying to maintain your current health, you probably won’t have to go to therapy as often. You might just want to go once every couple of months to make sure all systems are go. If you recently had surgery or you’ve been recovering from a knee injury or crunched-up shoulder, though, you’ll want to keep up your Physiotherapy in Calgary South. Injury prevention is the goal here. Your body is weak and unstable after an injury, and you’ll want to go and have your physiotherapist help it get back to normal strength. You can also have your physiotherapist put you on a “preventative” maintenance plan so that you can go less often but still keep the risk of injury low.
To address chronic pain and muscle weakness.
If you have chronic pain or weakness in your muscles, you’ll want to go to physiotherapy as often as you can. The therapy sessions can help prevent the pain from becoming worse, and the physiotherapist can help you do exercises in your day-to-day life that might help alleviate pain. You’ll also probably want to see a pain management doctor so that you can get some medications that can help manage your pain. And, if you have weakness in your muscles, you’ll want to go to physiotherapy as often as they recommend you go. Your physiotherapist can help you strengthen your muscles by prescribing exercises you can do at home, and they can teach you how to move your body in a way that helps put your muscles in the right place.
Bottom line: It’s up to you!
Really, the frequency of your visits is up to you and your experienced physiotherapist. You can go as often or as infrequently as you want (within reason). You don’t want to go so often that it feels like a chore, but you also don’t want to go too infrequently and fall behind on your treatment. It’s entirely up to you and your physiotherapist to figure out how often you should be going. Call Peak Health & Performance and get started on your Peak Health Physio treatment plan today.
A sharp pain begins in your lower back, shoots down one of your legs and makes it impossible to walk normally.
If this has happened to you or someone you know, it’s likely that you have sciatica—the medical term for a condition in which nerve roots in the spine are compressed. A typical case of sciatica will last for about two to six weeks if left untreated. Getting the right treatment early can speed up the recovery time by helping you avoid secondary complications such as muscle spasms and atrophy, weakness, and numbness. These professionals are trained to diagnose and treat problems with a patient’s nervous system, including the sciatic nerve and lumbar spine. Each profession has its own set of skills, but they both work to get you on the road to recovery fast. Here’s what you need to know before choosing between physiotherapy or chiropractic care:
What is the difference between a physiotherapist and a chiropractor?
Physiotherapists and chiropractors have similar backgrounds and training, so they both know how to deal with chronic pain disorders. They will both use physical examinations to diagnose disorders and pain signals. Their education, though, varies depending on the country they are in. In the United States, both professions require a minimum of a master’s degree. In Europe, only chiropractors need a master’s degree, while physiotherapists require a doctorate. If you see a chiropractor for sciatica, you can rest assured that he or she has the necessary training to treat it—as well as other neuromusculoskeletal disorders such as spinal stenosis, hip pain or joint pain.
Physiotherapists are trained to treat a wide range of conditions, including those related to the nervous system. They can help you recover from sciatica, but they may also work with you to prevent it. Chiropractors, on the other hand, are trained to treat the causes of a sciatica-like pain, but not the symptoms. A chiropractor might prescribe chiropractic treatment such as exercises to strengthen your core and lower back muscles, or recommend that you exercise in a pool (to avoid overusing your leg muscles).
How do physiotherapists treat sciatica?
Physiotherapists can help you recover from sciatica pain by administering treatments to help relieve the symptoms you are experiencing. Depending on your specific pain, they might use ice packs to reduce swelling, heat packs to relax your muscles, or electrotherapy to reduce the pain in your nerves. They can also teach you how to exercise your core and lower back muscles, which can help you prevent a recurrence of sciatica. Physiotherapists can also work with you to modify your daily activities if you are experiencing a lot of discomfort when you are on your feet. Physiotherapists can also work with you to improve your posture and make sure that your workstation is ergonomically friendly. Improving your posture can help prevent a recurrence of sciatica by taking pressure off your lower back and core muscles. If you already have sciatica, good posture can reduce the pain.
How do chiropractors treat sciatica?
Chiropractors will examine your spine and lower limbs to find the cause of your sciatica. Once they’ve identified the source of your pain, they’ll use spinal manipulation to adjust the problematic joint to remove the pressure on your nerve roots and provide pain relief. Your chiropractor might also recommend a set of exercises to strengthen your core and lower back muscles, to prevent future episodes of sciatica. Depending on the severity of your symptoms, your chiropractor might prescribe an anti-inflammatory medication or muscle relaxants as part of your pain treatment.
Should you see a physiotherapist or chiropractor for sciatica?
Physiotherapists and chiropractors have many things in common, but they also have some key differences. Both use manual therapy as their approach to treatment, but depending on your specific needs and circumstances, you might benefit more from seeing one profession over the other.
For example, if your sciatica is mild and you are looking for ways to relieve the pain and improve range of motion, you should see a physiotherapist. If you have a moderate case of sciatica and want to speed up your recovery, you might want to see a physiotherapist first and then see a chiropractor.
Which profession should you see first?
If you are suffering from a mild case of sciatica, visit a physiotherapist in Calgary first. He or she will help you to identify the cause of your pain, which will help you avoid it in the future. You can then visit a chiropractor for treatment, if necessary. If you have a more serious case of sciatica, it’s best to visit a doctor first. Your doctor can administer a diagnostic test, prescribe medication (if necessary), and recommend exercises that you can do at home. Once your pain has subsided, you can visit a physiotherapist or Chiropractor in Calgary South for advice on how to prevent a recurrence of sciatica in the future. Depending on the severity of your symptoms, you might want to visit both professions.
Bottom line
Physiotherapists and chiropractors are both trained professionals who can help you recover from sciatica. Depending on the severity of your symptoms, you might want to see one or both professions for treatment.Peak Health and Performance has caring, professional physiotherapists that can relieve your sciatica symptoms. Give us a call today to learn how we can best help you!
You might think of physiotherapy as something reserved for people with broken bones or other serious injuries, but it’s so much more than that. From sprained ankles to frozen shoulders—there are many common conditions that a physiotherapist can help you recover from that will improve your quality of life.
A physiotherapist is a muscular specialist who helps treat people with different types of injuries or conditions on a daily basis. Their role is to assist patients in relieving pain and regaining strength and mobility after an injury or surgery, while also identifying risk factors for future injuries and helping to prevent them from happening again.
This article outlines 9 common conditions that can be treated by physiotherapy:
1. Sprained Ankles
Sprains are overuse injuries that can happen to anyone, at any time. They occur when the soft tissue that connects your bones to your muscles (ligaments) is overstretched, which leads to a tear. This can cause swelling and severe pain, which can make walking or running very difficult—if not impossible. Depending on the severity of the sprain, you can usually recover in a few days to a few weeks.
A Peak Health physiotherapist can help to speed up your recovery by providing you with targeted exercises or stretches for your specific injury. Exercises are a great way to help strengthen your joint and surrounding muscles, making it easier to lift and push your foot off the ground when you walk. Sprained ankles can also be treated with a variety of different taping techniques that can help support your joint and keep it in proper alignment.
2. Frozen Shoulder
A frozen shoulder is also known as adhesive capsulitis. It causes your shoulder joint to stiffen, which leads to pain and limited range of motion. Frozen shoulder is more common in individuals over 40 and women who have had children.
A physiotherapist can help you manage your symptoms and regain range of motion by stretching out your tight muscles and providing you with exercises to help improve your strength and joint mobility. They may also use heat therapy, cold therapy, or ultrasound to help speed up the healing process. A physiotherapist can also assist you with a shoulder massage technique called joint mobilization, which helps increase the range of motion in your shoulder, while also reducing pain and stiffness. If your shoulder is frozen, it’s important to see a physiotherapist as soon as possible.
3. Scoliosis
Scoliosis is a curvature of the spine that causes a side-to-side imbalance in your spine. It is a common childhood condition, but can also develop later in life.
A physiotherapist can help you manage your symptoms and improve your posture with a special exercise called a “posture correction exercise”. This exercise can help reduce your scoliosis symptoms, improve your posture, and help you feel more comfortable while sitting and standing. If you have scoliosis, it’s important to see a physiotherapist to determine if you need to wear a back brace. A physiotherapist can assist you in choosing the right type of back brace for your condition. They can also help you fit and wear your back brace properly.
4. Knee Pain
Knee pain is a common complaint that often comes from overusing your joints, which can happen if you are a runner or someone who does a lot of heavy lifting. This can cause your knee joint to be overworked and lead to inflammation of the knee.
A physiotherapist can help you manage the pain and reduce inflammation with ice, heat, and other treatments. They can also help you with a number of different exercises, such as squats and lunges, to help strengthen and stretch your knee joint. If you have knee pain, a physiotherapist can help you determine if you have a torn meniscus or a knee ligament tear, which requires a different treatment plan. They can also test your knee joint mobility using a variety of different tests, such as the leg length test, to determine if you have knee joint restrictions.
5. Exercise Intolerance
Exercise intolerance is a condition that has to do with your heart and lungs. It makes it difficult for your body to get enough oxygen, which can cause you to get out of breath very easily. If you have exercise intolerance, you might find that you get out of breath quickly when climbing stairs or walking up a hill. This can make even the most basic daily activity difficult.
A physiotherapist can help you manage your symptoms and improve your overall fitness by prescribing a physical therapy and fitness program. They can also help you learn how to use an inhaler properly, if you have asthma. A physiotherapist can also help you make sure you are safe when exercising. They can assist you with a fitness assessment to determine which exercises are best for you, or find ways to modify exercises if you are at risk for injury. They can also help you find a safe way to exercise at home, if you have a physical impairment.
6. Chronic Back or Neck Pain
Back and neck pain are common conditions that can be caused by a number of different things, such as poor posture, heavy lifting, or an injury. Some back and neck pain resolves by itself after a few days or a week, but persistent back or neck pain may make daily living difficult. Some pain can only be relieved with the help of a physiotherapist.
A physiotherapist can help ease your chronic pain by creating a personalized exercise program designed for your specific condition. They can also help you improve your posture by identifying and correcting any bad habits or muscle imbalances in your upper or lower back. This can help reduce your chronic pain and put you on a path to reclaiming a pain-free life. If you have chronic pain, a physiotherapist can determine your pain levels and assist you with a specific exercise program to help you manage the pain. They can also help you identify any potential injury or cause of your pain, and help you avoid re-injuring yourself. If your pain is chronic, it is important to see a physiotherapist as soon as possible, as waiting too long can make it harder to recover.
7. Sciatica
Sciatica is a painful malady that’s caused when the sciatic nerve is irritated. This vital nerve runs from your lower back, through your hips and down to your legs. It can be caused by a number of different things, such as a herniated disc, degenerative disc disease (DDD), or a spinal stenosis.
A physiotherapist can help you manage your pain and improve your mobility with a combination of targeted stretches and exercises. They can also assist you with heat therapy, cold therapy, and joint mobilizations. If you have sciatica, a physiotherapist can help you determine if you have a herniated disc or DDD, which affects your sciatic nerve, versus a spinal stenosis, which does not. If you have sciatica, it is important to see a physiotherapist as soon as possible, as waiting too long can prolong your recovery period.
8. Carpal Tunnel Syndrome
Carpal Tunnel Syndrome is a common wrist problem that occurs when your carpal tunnel swells, which causes pressure on the nerves in your wrist. This can lead to pain, tingling, and numbness in your hands and wrists.
A physiotherapist can help you manage your pain, improve your strength, and create a safe exercise program, as many people with carpal tunnel syndrome have trouble exercising. They can also help you with a number of different exercises designed specifically to reduce your pain, regain strength, and improve mobility in your wrists and hands. If you have carpal tunnel syndrome, a physiotherapist can help you determine if you need surgery to relieve pressure on your nerves. They can also help you recover from surgery and avoid re-injuring your wrists when you’re done healing.
9. Rotator Cuff Injury
A rotator cuff injury is when one of your shoulder muscles is injured.
A physiotherapist can help you recover from rotator cuff injuries, such as tears, by teaching you how to properly use your shoulder. They can also help you with a number of different exercises designed to improve your strength, range of motion, and help you avoid re-injuring your shoulder. If you have a rotator cuff injury, a physiotherapist can also help you determine if you need surgery to repair the injury, or assist you with managing your pain with other treatments. If you have a rotator cuff injury, it is important to see a physiotherapist as soon as possible, as waiting too long can make it harder to recover.
Wrap Up
Peak Health and Performance is a physiotherapy practice that has successfully treated these conditions and others in the Calgary community for years. Our caring, professional staff can guide you with an initial assessment that will diagnose the source of your problem and offer a personalized treatment plan designed to help you recover soon. Call Peak Health & Performance today to learn more about how physiotherapy can help you.
By: Dr. Claire Wells, DC
Chiropractor, Peak Health Elbow, Calgary, Alberta.
If you’ve ever had pain on the bottom of your heel, you’ve probably been told (or with the help of Dr. Google you’ve told yourself) that you have plantar fasciitis. And you could be right! In this post I’m going to break down the basics of this condition, and what we can do about it. Let’s dive in!
Anatomy Overview
When there is pathology in the plantar fascia, we are specifically referring to a section called the “aponeurosis.” Almost always, there is degeneration of this tissue, as opposed to inflammation. This means the term “fasciitis” is not very accurate (“-itis” indicating inflammation), and “fasciopathy” is more appropriate (“-opathy” indicating an injury or problem with a tissue).
The plantar aponeurosis originates from the calcaneal tubercle (a bump on the bottom of the heel bone) and extends to the forefoot. In the forefoot, it divides into five separate bundles, which attach to the closest part of the toes. The plantar aponeurosis is not identical to a tendon or a ligament – it’s somewhere in-between, and is comprised largely of type 1 collagen. (1)
Fascial Function
The plantar aponeurosis supports the bottom of the foot, especially the medial arch. It plays an important role in turning the foot into a rigid lever during the push-off (“propulsion”) phase of walking and running.(2) But it doesn’t work alone!Other structures support the medial arch as well, including muscles. Strength of these muscles is critical for foot stability, and for preventing the aponeurosis from being over-stressed. Eccentric strength, which is when a muscle is lengthened under load, is especially important, since walking and running involve a lot of joint deceleration.
When walking or running, the aponeurosis and the associated muscles become tensioned when the big toe extends. This is called the ‘windlass mechanism’ and is critical for efficient movement.(2) Ensuring that we have good range of motion and strength of the big toe is important for healthy plantar fascia.
So what is plantar fasciopathy?
The problem is excessive biomechanical strain at the insertion of the aponeurosis on the heel bone. When the demands on the tissue exceeds the tissus ability to heal, we get tissue breakdown, or degeneration, and sometimes pain. Inflammation does not typically occur.
What are the risk factors for developing plantar fasciopathy?
The following factors can be associated with plantar fasciopathy(3, 4). The bold ones are factors that are modifiable (which is great news!). It’s important to realize that if any of these apply to you, it does not mean that you will get plantar fasciopathy, nor does it mean that you can’t do anything about it if you do get it.
BMI >27
Excessive running or a recent significant increase in weight-bearing activity
Intrinsic foot muscle and calf muscle tightness
Reduced ankle dorsiflexion range of motion, and/or excessive plantarflexion range of motion
Weak calf muscles
Sedentary lifestyle
Metabolic conditions such as Type 2 Diabetes
Acute increase in loading/exercise
Leg length discrepancy
Femoral or tibial torsion (This means an excessive structural twisting of the thigh or shin bone; this is something that we cannot change. But having this anatomical variation does not mean you are doomed!)
Occupations that require prolonged periods of walking or standing
High arches
Low/flat arches
How Do I know if I might have plantar fasciopathy?
Classic signs of plantar fasciopathy include(3, 4):
Pain located at the bottom of the heel, or where your heel and arch intersect
Usually affects only one foot
Worse first thing in the morning, or with the first steps after being prolonged rest (especially if your ankle has been in plantar flexion, aka pointed downwards). It may also be worse in the evening.
Pain is sharp or stabbing, and does not radiate
No tingling or pins and needles
Do I need to get diagnostic imaging?
X-rays can’t help us, because this is not a bone problem. Ultrasound and MRI can show the density and thickness of the fascia, but we don’t need that information to diagnose the condition or predict prognosis. So, diagnostic imaging is not necessary unless other injuries like a fascial rupture or a calcaneal stress fracture are suspected.(4)
Differential Diagnoses: What else could my plantar heel pain be?
“Plantar” refers to the bottom surface of the foot. Not all pain on the bottom of the heel is plantar fasciopathy! Other causes of pain in this region can be misdiagnosed as plantar fasciopathy, and thus may end up being treated ineffectively. Peripheral nerve entrapment is a big one. This is when one of the nerves that supplies the bottom of the foot is compressed, or otherwise biomechanically irritated. If this is the cause, you might only get pain, but you might also get numbness, pins and needles, tingling, or burning or electric-like pain. You may also feel worse during or after stretching, or rolling out the bottom of the foot. Nerve pain could also be originating from the low back, so it’s important to rule out the spine as the culprit.Sometimes you can get plantar heel pain from muscle tightness or trigger points. Other less common conditions that can cause pain in this area include tibialis posterior tendon dysfunction, calcaneal stress fracture, insertional achilles tendinopathy, Sever’s apophysitis, calcaneal fat pad atrophy, and inflammatory arthropathy.
If I have plantar fasciopathy, what can I do about it?
Ensuring that you see a practitioner who can assess your specific case and prescribe an individualized exercise program for your mobility and stability needs is an important step in tackling your pain.
You may need initial activity modification to reduce pain, but gradual overload of the tissue is required to promote healing and build up capacity for loading. Being out of pain does not equal being ready to immediately dive right back into high activity levels.
Addressing factors that may have contributed to this in the first place is important. Do you have good foot stability and control? If not, you might rely too much on passive structures like the plantar aponeurosis. Do we have good trunk and lower limb stability and control? If not, the whole posterior chain may over-work and tense up, which may cause nerve or muscle tension as far down as the calf and foot.
Treatment Options for Plantar Fasciopathy
Usually for long-term success, we need to work on intrinsic foot muscle strength, and big toe mobility and strength.But when it comes to treatment that targets the plantar fascia itself, we have research-based exercise protocols that improve function and reduce pain. Keep in mind that because this is a degenerative condition of connective tissue (which takes longer to heal), you will have to be patient with the recovery process. It’s not going to go away within a few days!
When it comes to pain and function, we have a hierarchy of interventions.
Strengthening the plantar fascia is superior to…
Stretching the plantar fascia, which is in turn superior to…
Stretching the Achilles tendon/calf muscles
Good strengthening requires that we get tension in both the Achilles and the plantar aponeurosis, by activating the windlass mechanism. You’ll recall that the windlass mechanism is when big toe extension tensions the aponeurosis and muscles of the medial arch. We invite the Achilles tendon to the party to further increase fascial tension – this works because these two connective tissue structures are, well, connected! (1)
Where to Start:
Single leg calf raises, with the toes supported in maximal extension is a great place to start.(6) There is a specific loading protocol that research has shown to be effective, but it’s best to see your chiropractor or physiotherapist for an exercise program that is tailored to your specific needs. The studies on this used a 12-week program, which is important to keep in mind. It takes time for the tissue to adapt, even if you start to see improvement in pain before 12 weeks.
Shockwave therapy, laser therapy, orthotics, dry-needling, taping, and other techniques provided by chiropractors and physiotherapists can be helpful for improving pain and function, as adjuncts to exercise.
What about injections?
A systematic review and meta-analysis found no high-quality evidence to show that corticosteroid injections are better than other forms of treatment for improving pain and function in the short, medium, or long-term.(9) They have similar outcomes to placebo injections (which means that a real corticosteroid injection was not better than a fake one). They also result in total rupture of the fascia in 2-10% of cases.
A systematic review and meta-analysis of platelet-rich plasma (PRP) vs. corticosteroid injections found that PRP is better at reducing pain, however, the quality of the studies was generally low and the injection protocols were highly variable, so these results must be viewed with caution.(10)
Overall, I recommend trying conservative treatment first, such as chiropractic or physiotherapy. PRP may be something to consider for severe and/or chronic, unremitting pain.
Take-home points:
Plantar heel pain is not always plantar fasciopathy. Get assessed to make sure
The plantar aponeurosis needs help from the muscles of the foot, and good mobility of the big toe, in order to function well
Treatment may need to address more than just the foot itself
Strengthening is the best treatment! This tissue requires intentional loading to recover properly
References:
Stecco C, Corradin M, Macchi V, et al. Plantar fascia anatomy and its relationship with Achilles tendon and paratenon. J Anat. 2013;223(6):665-676. doi:10.1111/joa.12111
Wearing SC, Smeathers JE, Urry SR, Hennig EM, Hills AP. The pathomechanics of plantar fasciitis. Sports Med. 2006;36(7):585-611. doi: 10.2165/00007256-200636070-00004.
Trojian T, Tucker AK. Plantar Fasciitis. Am Fam Physician. 2019 Jun 15;99(12):744-750. PMID: 31194492.
Monteagudo M, de Albornoz PM, Gutierrez B, Tabuenca J, Álvarez I. Plantar fasciopathy: A current concepts review. EFORT Open Rev. 2018 Aug 29;3(8):485-493. doi: 10.1302/2058-5241.3.170080.
Menz HB, Thomas MJ, Marshall M, Rathod-Mistry T, Hall A, Chesterton LS, Peat GM, Roddy E. Coexistence of plantar calcaneal spurs and plantar fascial thickening in individuals with plantar heel pain. Rheumatology (Oxford). 2019 Feb 1;58(2):237-245. doi: 10.1093/rheumatology/key266. PMID: 30204912; PMCID: PMC6519610.
Rathleff, M. et al. “High‐load strength training improves outcome in patients with plantar fasciitis: A randomized controlled trial with 12‐month follow‐up.” Scandinavian Journal of Medicine & Science in Sports 25 (2015)
Riel H, Jensen MB, Olesen JL, Vicenzino B, Rathleff MS. Self-dosed and pre-determined progressive heavy-slow resistance training have similar effects in people with plantar fasciopathy: a randomised trial. J Physiother. 2019 Jul;65(3):144-151. doi: 10.1016/j.jphys.2019.05.011. Epub 2019 Jun 13.
Salvioli S, Guidi M, Marcotulli G. The effectiveness of conservative, non-pharmacological treatment, of plantar heel pain: A systematic review with meta-analysis. Foot (Edinb). 2017 Dec;33:57-67. doi: 10.1016/j.foot.2017.05.004. Epub 2017 Jun 15. PMID: 29126045.
Whittaker GA, Munteanu SE, Menz HB, Bonanno DR, Gerrard JM, Landorf KB. Corticosteroid injection for plantar heel pain: a systematic review and meta-analysis. BMC Musculoskelet Disord. 2019 Aug 17;20(1):378. doi: 10.1186/s12891-019-2749-z. PMID: 31421688; PMCID: PMC6698340.
Hohmann E, Tetsworth K, Glatt V. Platelet-Rich Plasma Versus Corticosteroids for the Treatment of Plantar Fasciitis: A Systematic Review and Meta-analysis. Am J Sports Med. 2021 Apr;49(5):1381-1393. doi: 10.1177/0363546520937293. Epub 2020 Aug 21.
Running is one of the most accessible forms of exercise, and a great way to enjoy being outside during these remaining weeks of good weather in Calgary. Because so many people run, there is a lot of information that circulates on social media, in marketing campaigns, and even by word of mouth, about what we “should” do when it comes to running. But not all information is good information, so below I bust four common running myths to help you get the most out of the season!
MYTH 1: “You should minimize rotation of the trunk and arms.”
When I started running, I was certain that rotating my body was bad. I was told it was a waste of energy; that my arms should never stray from straight, and my hips should always face perfectly straight forward. I was so proud when I would go for a run and keep my trunk super rigid and stiff.
But wow, was I wrong! As it turns out, running is a rotational sport. Controlled rotation throughout the body is how we propel ourselves forward. Let me explain…
It would be easy to think of the legs as being our primary drivers for moving our body forwards when we run (after all, that’s what it looks like!). But even if you had no legs, you would be able to “walk” by reciprocal rotation of the pelvis (driven by the lumbar spine, AKA the low back) and the shoulders (driven by the thoracic spine AKA the mid and upper back).
[Image1]
“It’s important to realize that trunk, hip, knee, ankle, and foot rotation is normal and necessary to run efficiently. And efficiency means reduced injury risk.”
This is not to say that the legs don’t matter! Even though the trunk is our driving force, the legs play a huge role in running, and they also must rotate. It’s important to realize that trunk, hip, knee, ankle, and foot rotation is normal and necessary to run efficiently, which means reduced injury risk.
Now, this doesn’t mean we should go out and run like a wacky inflatable tube man, flailing our body parts into twisting motions. There is such a thing as unhelpful rotation (if it’s not producing momentum to propel us forward, it’s not helpful), so there is a sweet spot when it comes to how much rotation we produce at each level of the body. And most importantly, if we do not have control of the ranges we use when running, we are setting ourselves up for some problems.
[Image2]
My Advice:
Be able to resist rotation before you can expect to create it efficiently and be able to control the range of motion available to you. This means doing specific exercises to build up your capacity (and yes, you need to strength train if you are a runner!). It’s best to see a chiropractor or physiotherapist in Calgary who can identify deficiencies specific to you, and prescribe exercises accordingly but here are a few examples:
• Core/trunk: Paloff press, bear plank or high plank shoulder taps, cable chops and lifts
• Hip: single leg Romanian deadlifts, hip airplanes, 90-90 get-downs, rotational cable squats
• Ankle and foot: banded supinations, ankle rocker board, active inversion-eversion
Unlike me when I started running, don’t think you need to keep your shoulders and hips rigidly facing forward when you run. Let your “spinal engine” do its thing!
MYTH 2: “You should forefoot strike to reduce impact on your joints”
You may have heard that landing on your heel is “bad for your joints,” or even just that it’s inefficient. Don’t believe the lies, friends! There is no inherently superior strike pattern during running.
Our bodies are smart, not to mention highly variable in individual anatomy, and your body will self-select the strike pattern that is mechanically efficient for you. Speed of running will also change this. Until you reach a 6:00-6:30 minute-mile pace, heel striking is more efficient for most people. At that pace, heel and midfoot striking are about equally efficient. Most elite marathoners midfoot strike because they are running so fast. Similarly, you’ll notice that sprinters are always landing on the forefoot, out of necessity, because of their speed.
Slow running is more efficient with heel striking. This means runners who naturally heel strike should not try to intentionally forefoot strike. Doing so may overload the gastrocnemius (not as well designed to absorb force) and can lead to posterior calf (and Achilles tendon) injury.
[Image3]
When we change our strike pattern, we change what structures are predominantly absorbing the force, but we do not change how much force the body needs to absorb. [4]
• Forefoot strike: ankles and calves
• Midfoot strike: foot arches and tibialis posterior
• Heel strike: knees and tibialis anterior
So, good news: There is no difference in injury rate between forefoot and rearfoot striking, and there is no association between foot strike pattern and performance. [2, 3, 7] Thus, no need to force yourself to change what you do.
Note: I am not advocating that everyone heel strike, just recommending that you don’t try to intentionally change your heel strike pattern, unless you have significant knee pain, for example. But if that’s the case, see a chiropractor or physiotherapist!
My Advice:
What most research seems to support is that what we should care about, more than foot strike, is the angle of the tibia (the shin bone) when we make contact with the ground. We want to see at most a 7-degree angle in front of vertical. Vertical, as in the shin being perpendicular to the ground (or straight up from the foot to the knee), is ideal. Not sure if you do this? Try having someone film you running, take some screenshots, and then use a free app like Technique or Hudl to draw angles on the photo.
[Image4]
MYTH 3: “You should wear a supportive shoe to minimize risk of injury”
Ultra-cushioned and motion-control shoes are becoming more popular because marketing campaigns have us believing that they can better attenuate shock, and thus reduce injuries. But…do they? Let’s take a look at some research…
[Image5]
“Extra cushioning interferes with proprioception, and therefore slows reaction time. This means our ability to stabilize and control our lower extremity is compromised, and you may get injuries higher up the chain.”
One study found that in the ultra-cushioned shoes, the timing was off for normal joint motion between the calcaneus (heel bone) and tibia (shin bone). This resulted in increased rotational stress on the knee, which may contribute to knee injury.
→ Super-cushioned shoes are unlikely to benefit your mechanics in a way that is protective or advantageous. [8]
One study followed 952 runners for a year. They all ran in a neutral running shoe, regardless of their foot type, and there was no significant difference in the risk of sustaining an injury for any foot type. This makes sense because foot type is NOT consistently associated with injury rates in research. [9]
In a study that followed runners training for a half-marathon, they found that those wearing the motion control shoes had significantly greater pain, regardless of foot type.
→ They concluded that picking shoes based on stability categories does not reduce the risk of running pain. [11]
This might go against what seems intuitive, which is that sloppy feet need to be controlled. But, excessive cushioning decreases the foot’s ability to get sensory information and send it to the brain. Reduced sensory input to the brain equals reduced quality of motor output (we can’t react to what we don’t know). We need constant feedback of impact forces and foot position to control ourselves. [10]
For this reason, it makes sense that wearing a highly motion-controlled or cushioned shoe could actually be WORSE for someone with feet that pronate too early or for too long. Extra cushioning interferes with proprioception, and therefore slows reaction time. This means our ability to stabilize and control our lower extremity is compromised, and you may get injuries higher up the chain.
My Advice:
The take home here is that you don’t need a specific type of shoe for a specific type of foot. Just buy shoes that feel COMFORTABLE. Your toes should be able to splay within the shoe, so if you can get a wide toe box on your shoes, even better.
MYTH 4: “You should stretch to prevent injuries”
NO studies have shown that “acute stretching,” aka stretching right before a run, improves running performance. It might actually decrease it! And long-term stretching doesn’t seem to make for better running, either.
Here are some brief examples based on research: [12]
• Stiffer thigh and calf muscles equals better force transfer between the deceleration and push-off phases.
• Less flexible hip and calf means less muscular effort needed to stabilize during foot strike
• 10 weeks of stretching resulted in no improvement in running efficiency, and no reduction in injury incidence. In this case, the stretching was even done separately from running.
• Gene COL5A1 is associated with inflexibility, and is found in elite endurance (runners with this gene had significantly higher running efficiency than others in one study)
• Stretching has no effect on chronic injury prevalence in runners
[Image6]
Elastic energy is what makes running efficient. The changes that occur from stretching reduce our ability to store and release elastic energy. So, we need more muscular effort to stabilize our joints.
High muscular effort = more oxygen needed = it takes more work to run!
This applies to stretching right before a run, and also long-term. Now, this doesn’t mean nobody should stretch. It really depends on how much range of motion you already have (and control of that motion, like I mentioned in Myth 1). There is a sweet spot, where you have enough range of motion to allow for the required movement, but not so much that we sacrifice elastic energy.
Another interesting thing to note is that there is also no evidence that stretching has the ability to reduce the severity or duration of delayed onset muscle soreness (DOMS). So, for most of us, stretching is not going to prevent injuries, increase performance, or reduce soreness. But sometimes it feels good to do!
My Advice:
Go ahead and stretch if it feels good for you, but I’d recommend against doing a ton of it, and definitely not before a run, in the name of mechanical efficiency. Your time could be better spent on other activities to support your running goals.
Take-home points:
1. Let your body rotate while running
2. Don’t force a specific foot strike
3. When choosing shoes, just go with what feels comfortable
4. Stretching does not make you faster or less likely to be injured
These are general principles that will apply to most people, but if you are a runner and you’re experiencing pain or have questions about what running factors are specific to you, it’s best to get assessed by a chiropractor or physiotherapist. Our teams at Peak Health Elbow and Peak Health Marda will get you back to that runner’s high and you can book online here.
References:
1. Gracovetsky, Serge. (1997). Linking the spinal engine with the legs: a theory of human gait. Movement, Stability and Low Back Pain – The Essential Role of the Pelvis.
2. Kasmer ME, Liu XC, Roberts KG, Valadao JM. The Relationship of Foot Strike Pattern, Shoe Type, and Performance in a 50-km Trail Race. J Strength Cond Res. 2016 Jun;30(6):1633-7. doi: 10.1519/JSC.0b013e3182a20ed4. PMID: 23860289.
3. Kasmer ME, Liu XC, Roberts KG, Valadao JM. Foot-strike pattern and performance in a marathon. Int J Sports Physiol Perform. 2013 May;8(3):286-92. doi: 10.1123/ijspp.8.3.286. Epub 2012 Sep 19. PMID: 23006790; PMCID: PMC4801105.
4. Kleindienst F, Campe S, Graf E, et al. Differences between fore- and rearfoot strike running patterns based on kinetics and kinematics. XXV ISBS Symposium 2007, Ouro Preto, Brazil.
5. Hasselman C, Best T, Seaber A, et al. A threshold and continuum of injury during active stretch of rabbit skeletal muscle. Am J Sports Med. 1995;23:65-70
6. Cunningham C, Shilling N, Anders C, et al. The influence of foot posture on the cost of transport in humans. J Experimental Biol. 2010;213:790-797.
7. Miller R, Russell E, Gruber A, et al. Foot-strike pattern selection to minimize muscle energy expenditure during running: a computer simulation study. Annual meeting of American Society of Biomechanics in State College. PA 2009.
8. Brianne Borgia, Julia Freedman Silvernail & James Becker (2020): Joint coordination when running in minimalist, neutral, and ultra-cushioning shoes, Journal of Sports Sciences, DOI: 10.1080/02640414.2020.1736245.
9. Nielsen RO, Buist I, Parner ET, Nohr EA, Sørensen H, Lind M, Rasmussen S. Foot pronation is not associated with increased injury risk in novice runners wearing a neutral shoe: a 1-year prospective cohort study. Br J Sports Med. 2014 Mar;48(6):440-7. doi: 10.1136/bjsports-2013-092202. Epub 2013 Jun 13. PMID: 23766439.
10. Richards, C E; Magin, P J; Callister, R (2009). Is your prescription of distance running shoes evidence-based?. , 43(3), 159–162. doi:10.1136/bjsm.2008.046680.
11. Ryan MB, Valiant GA, McDonald K, et alThe effect of three different levels of footwear stability on pain outcomes in women runners: a randomised control trialBritish Journal of Sports Medicine 2011;45:715-721.
12. Claire Baxter, Lars R. Mc Naughton, Andy Sparks, Lynda Norton & David
Bentley (2016): Impact of stretching on the performance and injury risk of long-distance
runners, Research in Sports Medicine, DOI: 10.1080/15438627.2016.1258640
Most of us have been there before. You go to pick something up off of the floor and there it is. Back pain so severe you feel like you may never be able to walk again. An alternative scenario is pain that won’t stop nagging throughout your workday. You could also be someone who notices a ‘twinge’ every time you attempt a back squat. Regardless of the situation, a LOT of people experience back pain. If you haven’t, you are one of the lucky ones in the minority. The good news is, with proper understanding and management, it doesn’t have to define you! If any of this sounds familiar to you, the information below will be of benefit. You will gain a better understanding of back pain, how to manage it, and how to prevent it.
What is Mechanical Low Back Pain?
Starting with a very general overview of the anatomy of the lumbar spine (low back), it consists of 5 vertebrae, separated by intervertebral discs. The vertebrae provide structural support, guide movement, and provide protection for your spinal cord and spinal nerves. Your intervertebral discs provide shock absorption from impact activity and bending. Your lumbar spine also has various ligaments and muscles that contribute to structural support and movement. As you can see in the second image below, there is close interaction between the areas above and below your spine due to the overlap of multiple ligaments and muscles. These muscles help facilitate movement of your low back in 3 different planes:
Flexion/extension (forward/backward)
Lateral flexion (side bending)
Rotation (twisting)
Mechanical low back pain (also referred to as non-specific low back pain) is defined as “low back pain not attributed to recognizable, known specific pathology”3. As the name and definition suggest, you cannot conclusively determine the structure at fault for mechanical low back pain. Many research studies have indicated that even imaging (x-ray, CT scan, MRI) does not always correlate with clinical findings when it comes to low back pain. To hammer this point home, one of my mentors and colleagues used to say, “we could sit down and drink a few pitchers of beer arguing what we think the specific cause of mechanical low back pain is”.
When your low back pain is being assessed, the first step is to rule out any specific/serious causes of your pain. Examples of this include, but are not limited to, radiculopathy (nerve related deficits), cauda equina syndrome, tumor, fracture, infection, and inflammatory disease. If these more specific causes are ruled out, it is then labelled as non-specific mechanical low back pain. You may be asking yourself “how can a physiotherapist help if they cannot identify the cause of my back pain?”. The goal of assessment/treatment with a physiotherapist will be to manage the symptoms and identify contributing factors that may have led to the development of it in the first place.
Potential contributing factors to the development of your low back pain3,4:
– History of trauma
– Strain or overuse
– Postural dysfunction
– Dysfunction above and below the low back (mid back, pelvic girdle, hips)
– Core weakness or muscle imbalances
– Psychological factors (ex. fear of movement, depression)
– Work environment
– Pregnancy
Since mechanical low back pain is so common, there has been a significant amount of research surrounding it, producing clinical practice guidelines (best practices) for diagnosis and management. A stratified approach is now most commonly suggested. The recommendations for management of your low back pain will differ depending on what group or subgroup you are categorized into. These groups/subgroups are usually based on chronicity of your back pain (acute, sub-acute, chronic) and presence of external factors that may contribute to it (psychological, work environment, etc.)1,3,4,6.
Why is it Important to Understand Mechanical Low Back Pain?
Low back pain affects 60-80% of individuals at some point in their lifetime3. Of these people, over 90% that present to a primary care practitioner have non-specific mechanical low back pain4. Back pain is also a significant economic burden to society. It is reported that the cost of care for low back pain is $50 billion annually in the United States4. Up to 23% of the world’s adults suffer from chronic low back pain (lasting longer than 3 months), which requires significant health care costs3. Without diving too deep into politics, in Canada’s public health care system and considering the significant costs associated with back pain, you could certainly argue it affects us all.
It is important to note that low back pain tends to be a self-limiting condition. Half of individuals will recover from it in 2 weeks without treatment, and the majority of individuals will recover in 1-4 months without treatment4. Although this is true, the recurrence rate of low back pain is high. 60% of people are likely to experience another episode of low back pain within 3-6 months4. These statistics indicate why it is important to see a rehab professional. First, some guidance will give you a higher likelihood of recovering in a shorter time frame. Second, education on your back pain will allow you to take preventative steps to decrease the likelihood of recurrent episodes.
As mentioned earlier, current guidelines take a stratified approach to diagnosing and treating mechanical low back pain. Depending on where you are categorized, the treatment may differ slightly. However, within each category, a few common themes exist. First, one of the most important aspects of care is providing reassurance and education. The better you understand your low back pain, the better you will be equipped physically and psychologically to deal with the pain. Second, exercise therapy and maintaining an active lifestyle is a key component to preventing and managing it. When it comes to mechanical low back pain, as long as a primary care practitioner has ruled out red flags, it is safe to move, and encouraged to help recovery. Finally, a multidisciplinary approach to low back pain management is recommended. This could include (but is not limited to) pharmaceuticals, psychology, conservative care, and self management1,2,4,5.
Some Risk Factors for Developing Mechanical Low Back Pain4:
– Pain, ache, or stiffness in the lumbosacral region (small of your back)
– Pain may radiate into your buttocks or upper leg (more often one sided)
– Pain may come on due to a specific event (bend, lift) or insidiously (gradual, no cause)
– Pain will increase or decrease with positional changes, certain movements, or lifting
– NO signs of Red Flags (i.e. significant trauma, unexplained weight loss, widespread neurological issues)
– NO known specific pathology (i.e. fracture, infection)
*Remember that these are the most common symptoms that would indicate you may have mechanical low back pain. It may present with different signs/symptoms depending on the individual. If this sounds like you, reach out to a Peak Health physiotherapist or another health care practitioner for a thorough assessment to determine the cause of your specific symptoms.
3 Strategies to Help Manage Your Mechanical Low Back Pain Symptoms
1. Keep it Moving
*Movement and activity are a key component to recovery and prevention of mechanical low back pain. Pick an activity you like to do (yoga, walking, cycling) and do it within the limits of your pain levels. You may have to modify the activity in the short term, but the movement will be beneficial for your body.
2. Low Back Mobility
*Working on mobility in your lumbar spine will help decrease pain levels and encourage more efficient movement in the long term. Try 3 sets of 10-15 repetitions.
3. Back/Core Strengthening and Motor Control
*Strength and coordination of the back, hip, and core muscles will allow you to get back to normal activity sooner and prevent episodes of back pain in the future. Try 3 sets of 8-10 repetitions on each side.
FAQ
How Do I Relieve My Low Back Pain?
It is best that you take an active approach or incorporate movement to help alleviate your back pain. Another suggestion includes using heat or ice to help decrease pain or muscle spasm. Clinical practice guidelines also recommend short term use of over-the-counter anti-inflammatory medications. However, it is best to consult a physician or pharmacist prior to use to ensure medication is safe and effective for you.
When Should I Be Worried About My Low Back Pain?
If your low back pain is non-specific mechanical low back pain, there is no need to be worried, as your pain will likely resolve with multimodal treatment. Mechanical low back pain is self-limiting, and it is usually safe to resume activity as tolerated. However, it is best to have it assessed by a physiotherapist or another health care professional in order to rule out red flags or specific causes of your pain that may require more immediate attention.
How Should I Sleep With Low Back Pain?
Most comfortable sleeping position will vary from person to person and there is no right or wrong answer. You may have to try a few different positions to find out what is best for you. One option to try is sleeping on your back with a pillow supporting your knees. Another option is sleeping on your side with a pillow between your legs. These options can put your pelvis and low back in a position that may relieve some discomfort.
What Comes Next?
Remember, mechanical low back pain is not attributable to any recognizable or specific pathology. It is one of the most common complaints to primary care practitioners and has a large burden on the health care system. Mechanical low back pain can be complex and multifactorial. It usually requires individualized management using a stratified approach. Education, an active lifestyle, and multidisciplinary management will aid in more successful outcomes.
Start by trying some of the strategies listed above and see how it goes! Afterwards, it would benefit you to see a physiotherapist to guide you through treatment, depending on your response.
Feel free to reach out if you have any additional questions on mechanical low back pain, or you can book an appointment online by clicking here.
References:
Almeida, M., Saragiotto, B., Richards, B., & Maher, C. G. (2018). “Primary care management of non-specific low back pain: key messages from recent clinical guidelines”. The Medical Journal of Australia, 208(6), 272–275. doi:10.5694/mja17.01152
Oliveira, C.B., Maher, C.G., Pinto, R.Z. et al. “Clinical practice guidelines for the management of non-specific low back pain in primary care: an updated overview”. European Spine Journal 27, 2791–2803 (2018). https://doi.org/10.1007/s00586-018-5673-2
Physiopedia 2021. “Low Back Pain”. Physiopedia. Accessed March 16, 2021, https://www.physio-pedia.com/Low_Back_Pain
Physiopedia 2021. “Non Specific Low Back Pain”. Physiopedia. Accessed March 16, 2021, https://www.physio-pedia.com/Non_Specific_Low_Back_Pain
Qaseem, A., Wilt, T.J., McLean, R.M., et al. “Noninvasive Treatments for Acute, Subacute, and Chronic Low Back Pain: A Clinical Practice Guideline From the American College of Physicians. Annals of Internal Medicine. (2017) ;166:514-530. [Epub ahead of print 14 February 2017]. doi:10.7326/M16-2367
Royal Dutch Society for Physical Therapy (2013). “KNGF Guideline: Low Back Pain”. Koninklijk Nederlands Genootschap voor Fysiotherapie, KNGF. http://www.ipts.org.il/_Uploads/dbsAttachedFiles/low_back_pain_practice_guidelines_2013.pdf
Media References:
Anatomy Pictures:
Click Physiotherapy (N.D.). “Lower Back Pain: Exercises and Stretches”. Accessed March 19, 2021 via Google Image Search. https://clickphysiotherapy.blogspot.com/2019/01/lower-back-pain-exercises-and-stretches.html [Original Source Unknown]






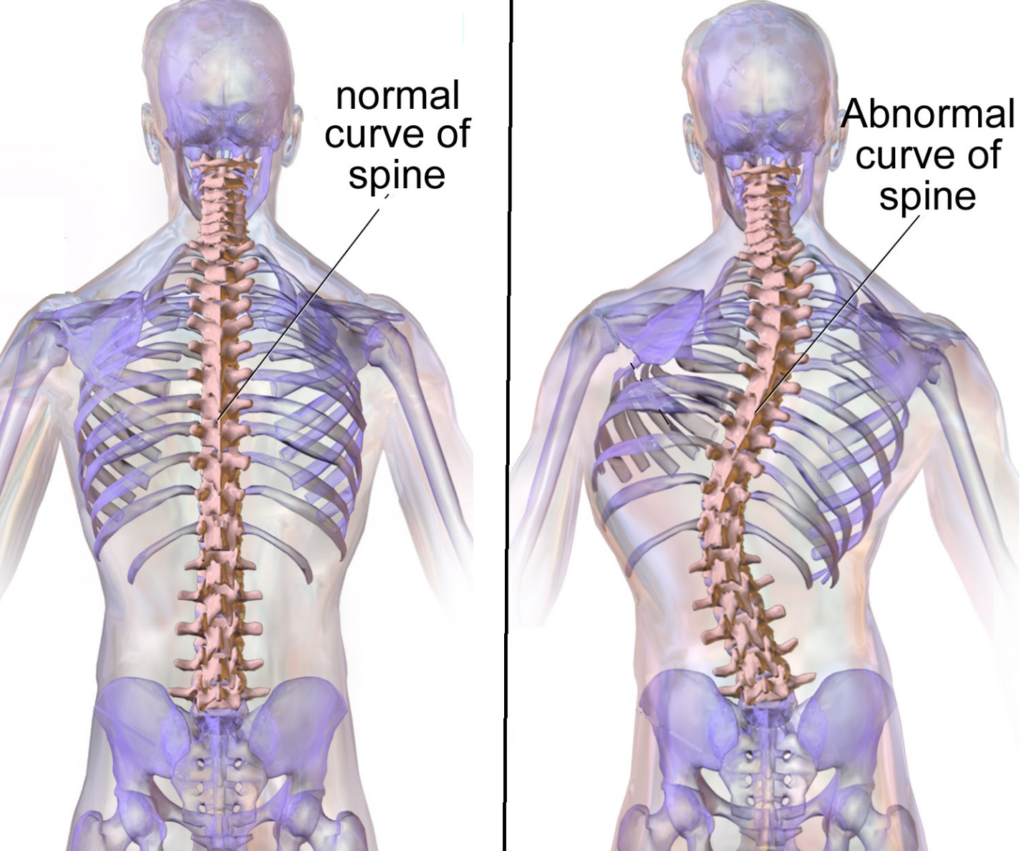
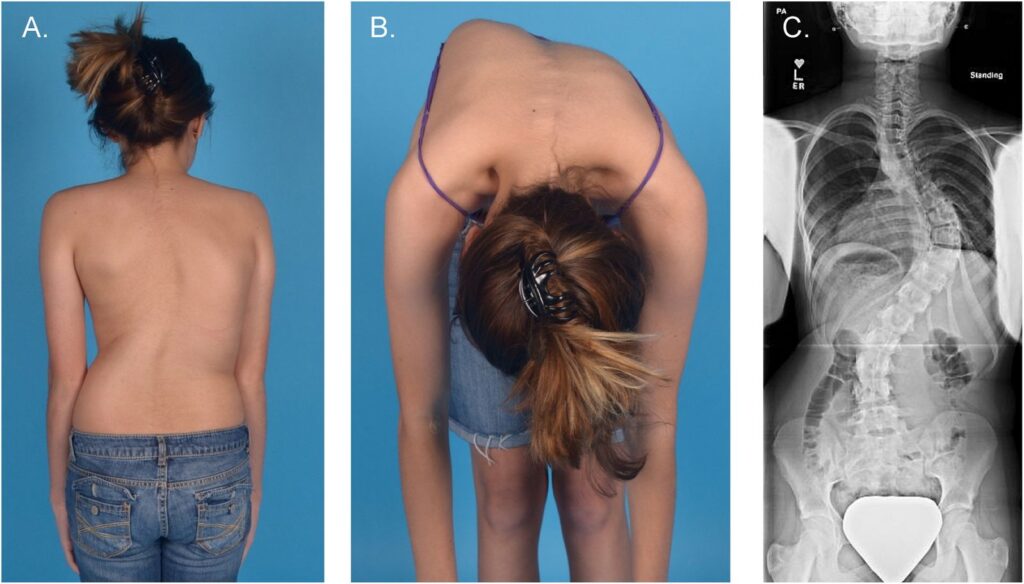







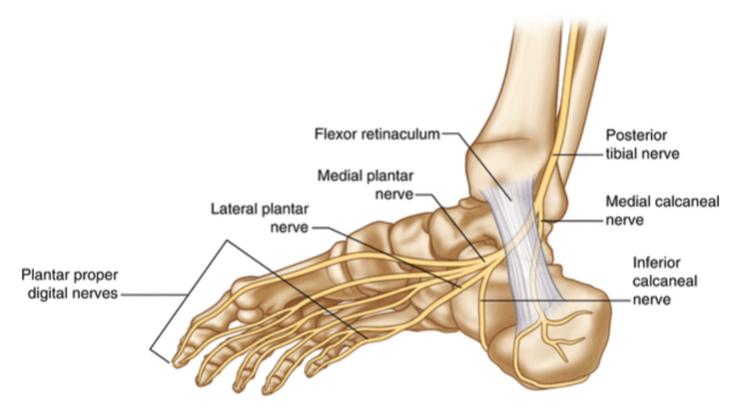

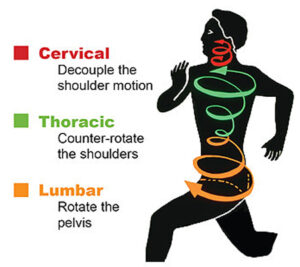
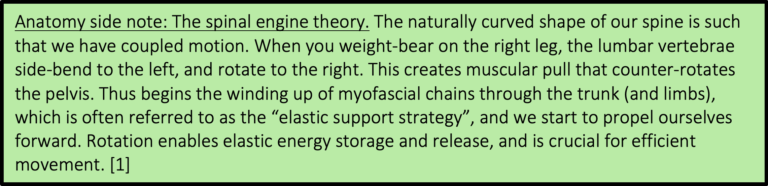

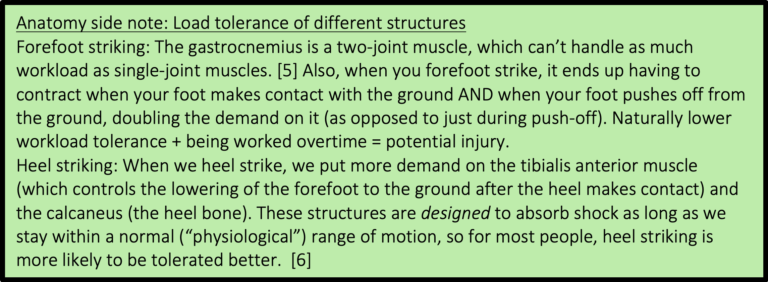

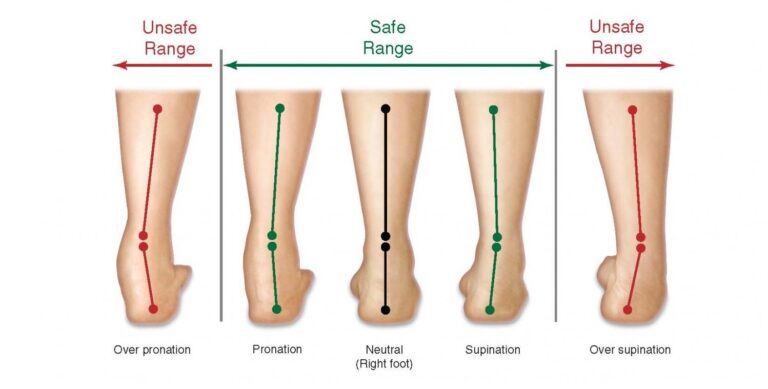


 Regardless of the situation, a LOT of people experience back pain. If you haven’t, you are one of the lucky ones in the minority. The good news is, with proper understanding and management, it doesn’t have to define you! If any of this sounds familiar to you, the information below will be of benefit. You will gain a better understanding of back pain, how to manage it, and how to prevent it.
Regardless of the situation, a LOT of people experience back pain. If you haven’t, you are one of the lucky ones in the minority. The good news is, with proper understanding and management, it doesn’t have to define you! If any of this sounds familiar to you, the information below will be of benefit. You will gain a better understanding of back pain, how to manage it, and how to prevent it.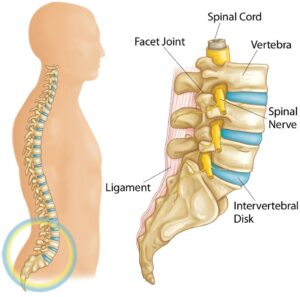
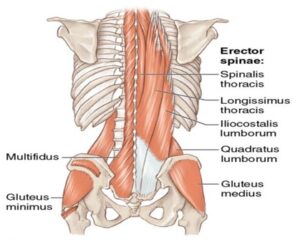
 specific/serious causes of your pain. Examples of this include, but are not limited to, radiculopathy (nerve related deficits), cauda equina syndrome, tumor, fracture, infection, and inflammatory disease. If these more specific causes are ruled out, it is then labelled as non-specific mechanical low back pain. You may be asking yourself “how can a physiotherapist help if they cannot identify the cause of my back pain?”. The goal of assessment/treatment with a physiotherapist will be to manage the symptoms and identify contributing factors that may have led to the development of it in the first place.
specific/serious causes of your pain. Examples of this include, but are not limited to, radiculopathy (nerve related deficits), cauda equina syndrome, tumor, fracture, infection, and inflammatory disease. If these more specific causes are ruled out, it is then labelled as non-specific mechanical low back pain. You may be asking yourself “how can a physiotherapist help if they cannot identify the cause of my back pain?”. The goal of assessment/treatment with a physiotherapist will be to manage the symptoms and identify contributing factors that may have led to the development of it in the first place. people, over 90% that present to a primary care practitioner have non-specific mechanical low back pain4. Back pain is also a significant economic burden to society. It is reported that the cost of care for low back pain is $50 billion annually in the United States4. Up to 23% of the world’s adults suffer from chronic low back pain (lasting longer than 3 months), which requires significant health care costs3. Without diving too deep into politics, in Canada’s public health care system and considering the significant costs associated with back pain, you could certainly argue it affects us all.
people, over 90% that present to a primary care practitioner have non-specific mechanical low back pain4. Back pain is also a significant economic burden to society. It is reported that the cost of care for low back pain is $50 billion annually in the United States4. Up to 23% of the world’s adults suffer from chronic low back pain (lasting longer than 3 months), which requires significant health care costs3. Without diving too deep into politics, in Canada’s public health care system and considering the significant costs associated with back pain, you could certainly argue it affects us all. treatment may differ slightly. However, within each category, a few common themes exist. First, one of the most important aspects of care is providing reassurance and education. The better you understand your low back pain, the better you will be equipped physically and psychologically to deal with the pain. Second, exercise therapy and maintaining an active lifestyle is a key component to preventing and managing it. When it comes to mechanical low back pain, as long as a primary care practitioner has ruled out red flags, it is safe to move, and encouraged to help recovery. Finally, a multidisciplinary approach to low back pain management is recommended. This could include (but is not limited to) pharmaceuticals, psychology, conservative care, and self management1,2,4,5.
treatment may differ slightly. However, within each category, a few common themes exist. First, one of the most important aspects of care is providing reassurance and education. The better you understand your low back pain, the better you will be equipped physically and psychologically to deal with the pain. Second, exercise therapy and maintaining an active lifestyle is a key component to preventing and managing it. When it comes to mechanical low back pain, as long as a primary care practitioner has ruled out red flags, it is safe to move, and encouraged to help recovery. Finally, a multidisciplinary approach to low back pain management is recommended. This could include (but is not limited to) pharmaceuticals, psychology, conservative care, and self management1,2,4,5.
 – Pain may radiate into your buttocks or upper leg (more often one sided)
– Pain may radiate into your buttocks or upper leg (more often one sided)